By Independent News Roundup
By Independent News Roundup

In highly Covid-19 (C-19) vaccinated populations, ongoing immune selection pressure is driving the emergence of increasingly infectious and dangerous SARS-CoV-2 (SC-2) variants. As a result of mass C-19 vaccination during the SC-2 pandemic—and the repeated breakthrough infections that followed in C-19 vaccinated individuals—a vicious cycle of immune escape has developed. In this cycle, the virus ultimately manages to evade not only the adaptive immune system but also the innate immune defenses of C-19-vaccinated individuals. According to the author, this process will culminate in the emergence of what he calls HIVICRON: a new variant—or potentially a new coronavirus—that is highly virulent for a large, vulnerable segment of the C-19-vaccinated population, capable of spreading rapidly within highly vaccinated communities and likely to trigger a wave of hyperacute mortality, particularly among those with prior breakthrough infections or long Covid.
Voice for Science and Solidarity by Geert Vanden Bossche is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
By contrast, unvaccinated individuals avoid exerting selective pressure on the virus due to training of their cell-mediated innate immune system. As a result, they are better equipped to continue defending against SC-2 variants and other respiratory viruses.
The author predicts that HIVICRON will mark the end stage of this immune escape pandemic. As the number of C-19-vaccinated individuals declines due to mortality, the pandemic will, in his view, extinguish itself—accompanied by a parallel drop (and eventual disappearance) of C-19 symptoms and C-19-related mortality among the unvaccinated.
He concludes that misguided public health policies and reckless mass vaccination campaigns will ultimately be shown to have taken a heavy toll on human life, and that a full analysis of this damage—possibly aided by artificial intelligence—will one day be needed to objectively assess and accurately quantify the true scale of this public health disaster.
Full text
We are increasingly observing a homogenization of COVID-19 (C-19) symptoms in populations with high C-19 vaccination coverage (‘highly vaccinated” populations’). More and more vaccinated, but also unvaccinated individuals, are now experiencing symptomatic reinfections with SARS-CoV-2 (SC-2). These manifest either as mild symptoms—such as hoarseness—or evolve into more severe forms of COVID-19, including long COVID and even death. As a result, the impression arises that it is currently the virus itself—rather than the type of immunity (natural versus vaccine-induced)—that predominantly determines the onset and course of C-19 illness in these populations. Consequently, many are increasingly convinced that no meaningful distinction needs to be made between individuals vaccinated with C-19 vaccines (‘C-19-vaccinated’) and those who are unvaccinated, and that breakthrough infections in C-19-vaccinated individuals and infections in previously naturally infected, unvaccinated individuals can be grouped together under a single category. This view is reinforced by the growing assumption that both forms of pre-existing immunity—natural and vaccine-induced—provide comparable protection and show similar shortcomings in that protection.
In my humble opinion, this apparent clinical convergence is highly misleading. Although I do not have access to hard epidemiological data, I believe—based on my long-term and thorough analysis of the pandemic's evolution, including clinical symptomatology, virological characteristics, and immune responses within highly vaccinated populations—that, for example, the partial protection against infection observed in both C-19 vaccinated and unvaccinated individuals, which clinically manifests as mild upper respiratory symptoms such as hoarseness, is rooted in fundamentally different immunological mechanisms. As previously stated on multiple occasions, this protection in unvaccinated individuals can be attributed to epigenetically induced training of the cell-mediated innate immune system. In contrast, the milder symptomatology seen in C-19-vaccinated individuals is likely the result of an enhanced cytokine-mediated humoral immune response. As described earlier (https://voiceforscienceandsolidarity.substack.com/p/viral-gain-of-function-is-associated?r=y46t6; https://voiceforscienceandsolidarity.substack.com/p/when-the-first-line-of-immune-defense?r=y46t6), this represents the only remaining immune strategy that C-19-vaccinated individuals can still deploy to control the virus, after their adaptive immune system has already exhausted all its means in a desperate attempt to contain the infection. I also refer to this as the ‘humoral’ arm of the innate immune system, to distinguish it from the cell-mediated arm which—as I have explained repeatedly in the past—has been bypassed in many C-19-vaccinated individuals due to antibody-dependent enhancement of infection (ADEI), primarily triggered by Omicron and its descendants.
Meanwhle, the circulating variants remain highly infectious, which—in unvaccinated individuals with a poorly trained innate immune system (such as young children) and/or reduced overall health (e.g., due to underlying conditions or an unhealthy lifestyle)—can lead to persistent reinfections and long COVID. Long COVID, however, may also be caused by specific (sub)variants capable of suppressing the induction of antiviral cytokines. This is highly likely the case in C-19-vaccinated individuals, who—due to insufficient protection by their adaptive immune system—increasingly rely on enhanced induction of antiviral cytokines in an attempt to contain ongoing breakthrough infections caused by a broad and diversified spectrum of more infectious, circulating SC-2 (sub)variants capable of evading host immune responses. Exposure of C-19-vaccinated individuals to (sub)variants that, under selective pressure from such innate, variant-nonspecific immune mechanisms, have evolved to also escape the humoral arm of innate immunity, may indeed be sufficient to cause chronic immune dysregulation and associated immunological manifestations of long COVID, including tumor pathology. Moreover, it is reasonable to assume that accidental exposure of C-19-vaccinated individuals to a saltation variant[1] capable of broadly and strongly suppressing the production or activity of antiviral cytokines could, in itself, be sufficient to trigger a fatal SC-2 reinfection. In contrast, in unvaccinated individuals, such a lethal outcome would likely require a combination of exposure to a variant harboring cytokine-suppressing mutations and the presence of host-specific predisposing factors, such as insufficient innate immune training or immunological weakness due to poor health status.
Although both host-intrinsic loss of innate immune control and virus-induced innate immune dysregulation—such as suppression of interferon (IFN) signaling and innate immune refocusing—can lead to prolonged, replication-driven emergence and shedding of viral mutants, those mutants generated (via immunological refocusing) in chronically infected individuals who previously experienced breakthrough infections tend to be more ‘dangerous’ than those arising from chronic infections in individuals with insufficiently strong or suboptimally trained innate immunity. Why? Host-intrinsic loss of innate immune control is pre-existing and pathogen-nonspecific (e.g., related to age or poorly trained/weak innate immunity) whereas virus-induced innate immune dysregulation develops as an active viral strategy (e.g., mediated by viral proteins) in individuals who previously experienced breakthrough infections (BTIs), even in the presence of immunocompetent cells. This strategy aims to dysregulate key antiviral immune mechanisms, leading for example to MHC-I downregulation, IFN suppression, and disruption of cytokine secretion, thereby promoting the emergence of viral escape mutants and their prolonged shedding in these individuals.
It is therefore primarily C-19-vaccinated individuals with prior vaccine breakthrough infections (VBTIs) who, within highly vaccinated populations, face an increased risk of death following reinfection with circulating SC-2 variants. In such populations, ongoing VBTIs in C-19-vaccinated individuals lead—via immune refocusing—to compensatory immune mechanisms that are repeatedly circumvented under slowly but steadily increasing immune pressure. This occurs because selection driven by the aforementioned variant-nonspecific immune mechanisms gives rise to the emergence and dominance of new SC-2 variants capable of repeatedly evading the immune system’s adjusted responses. There can therefore, in my opinion, be no doubt that the mortality rate among C-19-vaccinated individuals in highly vaccinated populations exceeds that of the unvaccinated—regardless of the lethal side effects of the mRNA vaccines themselves. In my view, C-19-related mortality among C-19-vaccinated individuals will also increase more sharply in the near future compared to that in the unvaccinated. As noted earlier, variant-nonspecific immune selection[2] is likely to promote the spread of ever-emerging variants characterized by mutations that increasingly suppress humoral components of the innate immune system. This stands in stark contrast to the cell-mediated arm of innate immunity—particularly stimulated in unvaccinated individuals—which is not pathogen-specific but broadly targets infected or otherwise pathologically altered host cells, regardless of the nature of the pathogen. As a result, this form of innate immunity does not confer a selective advantage to any particular pathogen or group of pathogens (e.g., viruses). The suppression of humoral innate immunity by dominant immune escape variants could explain not only the ongoing proliferation and spread of newly emerging immune escape variants but also the increased circulation of other respiratory viruses such as influenza, RSV, and rhinoviruses, which under normal conditions also typically cause acute, self-limiting infections. However, given that the current viral landscape is largely dominated by SC-2 variants, it is, in my opinion, abundantly clear that SC-2 in particular will take advantage of the suboptimal protection resulting from weakened antiviral cytokine activity. Consequently, the likelihood is increasing that a new type of coronavirus will emerge in highly vaccinated populations—one that is not only highly infectious but also fully escapes both the adaptive and innate immune systems of exposed individuals. Such a virus would therefore spread rapidly and with high virulence across these populations. I therefore continue to predict that HI-VI-CRON (HIghly VIrulent omiCRON descendant) will become the inevitable endpoint of this immune escape pandemic.
I do indeed expect that HIVICRON will lead to a high death toll among C-19-vaccinated individuals in highly vaccinated countries. Unvaccinated individuals, by contrast, do not offer any selective advantage to viruses or variants that suppress cytokine-mediated immunity—even when they continue to shed virus for prolonged periods due to a persistent SC-2 infection with (long) COVID symptoms. Based on my current understanding of the viral evolutionary dynamics during this immune escape pandemic, they therefore cannot be regarded as future breeding grounds for HIVICRON. On the contrary, as the vaccinated segment of the population declines due to mortality, even a weakened or suboptimally trained cell-mediated innate immune system in unvaccinated individuals will increasingly prove capable of effectively combating SC-2 variants and other respiratory viruses. I therefore expect that the mortality wave among C-19-vaccinated individuals will trigger a rapid and marked decline in the number of reinfections among the unvaccinated, and consequently also in the number of long COVID cases and C-19-related deaths—until these eventually disappear.
If my analysis is correct, we will in the coming weeks and months observe increasingly clear immunological differences between C-19-vaccinated and unvaccinated individuals within highly C-19 vaccinated populations, with growing disparities in the incidence of long COVID and mortality.
Conclusion:
The end result, in my view, remains a major wave of hyperacute mortality among C-19-vaccinated individuals—particularly among those who experienced clinically significant breakthrough infections and/or suffer from long COVID—accompanied by a parallel decline, up to the disappearance, of COVID symptoms and C-19-related mortality among the unvaccinated.
The bottom line remains that HIVICRON will become the inevitable endpoint for highly vaccinated populations, while it is primarily the unvaccinated who will survive this health crisis without any significant C-19 symptoms. Only then will viral transmission come to a halt, bringing an end to these seven lean years.
I do not dare to speculate on the number of human lives that this misguided vaccination campaign and the short-sighted public health measures will ultimately have cost humanity. However, no dataset is too large to be thoroughly analyzed and quantified—although this will likely require, at the very least, the assistance of artificial intelligence.
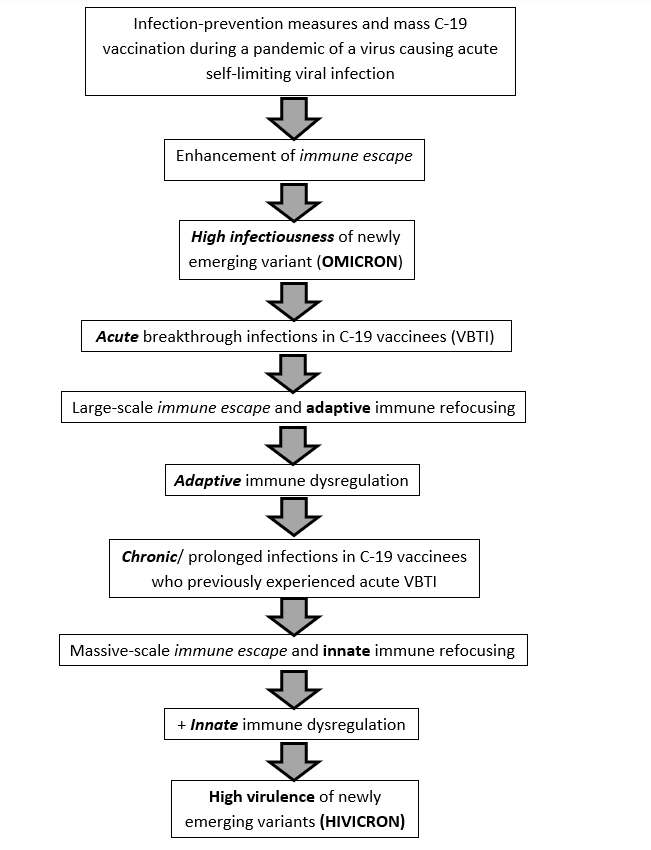
The diagram on the next page already illustrates how human inte4 | Pagervention in the original SC-2 pandemic enhanced viral immune escape, while progressively enabling more infectious immune escape variant to disrupt adaptive and eventually innate immune responses to the virus, inevitably leading to the high virulence of newly emerging variants, collectively referred to as 'HIVICRON’.
[1] A saltation variant is a viral variant that arises through a sudden, large-scale genetic change, characterized by an unusually high number of mutations appearing simultaneously, often in functionally important viral protein domains. Such variants typically do not emerge through gradual, selective accumulation of mutations over multiple transmission cycles, but rather may originate during prolonged infections in immunocompromised individuals or, in some cases, through zoonotic spillback
[2] In contrast to the replication-driven emergence of SC-2 mutants in permissive hosts where insufficient innate (and adaptive) antiviral responses allow extensive viral replication and accumulation of broadly diversified mutations through stochastic error-prone replication, innate immune escape variants emergence in highly C-19-vaccinated populations as a result of variant-nonspecific immune selection pressure exerted by suboptimal cytokine-mediated immunity in C-19 vaccinees