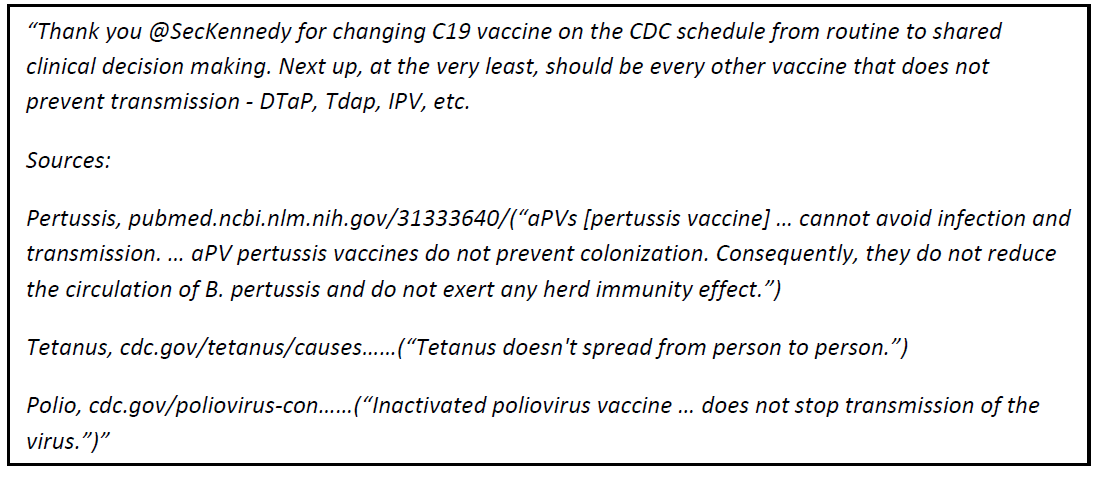
Regarding his comments on removing vaccines that do not prevent transmission:
Give
me a break! I can only hope that the next ACIP will not be composed of
lawyers. A. Siri has heard the clock toll but does not exactly know
where the clapper hangs. Let me educate him a bit on vaccinology: First and foremost, I want to point out that vaccines which, independently of their mode of administration, prevent transmission and thus infection simply do not exist. Such vaccines would have to exert sterilizing immunity to completely prevent productive infection. Nevertheless, it is perfectly possible
with some existing vaccines — even though they lack sterilizing
immunity — to prevent infection and transmission; however, this is only
achievable for acute, self-limiting infections where antibodies (Abs)
are a correlate of protection. By vaccinating
prophylactically, high Ab titers can be induced that neutralize viruses
causing such acute, self-limiting infections. This
protection, however, lasts only as long as the Ab titers in the blood
remain above a neutralizing threshold (comparable to the minimum
therapeutic concentration of a drug!). Once titers fall below this
neutralizing concentration, vaccine-induced Abs are no longer capable of
preventing infection and transmission. Does this mean that these vaccines become worthless at that point? Absolutely not! When
an immunologically naïve person has been primed, high Ab titers will be
rapidly recalled upon exposure, enabling disease prevention and
effective containment of transmission — just as happens with reinfection
following prior natural infection (and immunity). Thus,
no ‘suboptimal’ immunity arises; the disease duration will be very
short and mild, and vaccination will not lead to asymptomatically
infected individuals who could ‘silently’ transmit the pathogen and
serve as a reservoir for immune escape variants, thereby preventing the
population from establishing protective herd immunity. Asymptomatic carriers and the risk of sustained transmission and immune escape are also generated when perfectly preventive vaccines are used incorrectly,
for example by priming an entire immunologically naïve population
already exposed to the virus (see mass COVID-19 vaccination during the
pandemic!), or when vaccines are employed that—even under optimal
conditions (e.g., prophylactic administration and boosting to induce
high Ab titers)—cannot prevent the infectivity of the pathogen because
the nature of the induced immunity can only limit infection but not
prevent it entirely. This is, indeed, the case with pertussis
vaccination, and here I agree with A. Siri that large-scale immunization
programs against pertussis will simply make things worse in that we’ll
pay the price of symptom mitigation with persistent transmission and
pathogen immune escape. The same applies to streptococcal vaccination. There is, therefore, no scientific rationale to recommend these vaccines, let alone make their administration mandatory.
However,
immune escape is actually beneficial for the vaccine industry, since
the emergence of new variants allows antigenic components to be swapped
or newly added via simple cut-and-paste processes, facilitating rapid
production of new vaccines through existing procedures. In vaccinology,
there is a key principle that states, ‘the vaccine is only as good (or as bad) as the antigen.’
This principle is particularly relevant for chronic infections. If
these are targeted with the current vaccine concepts and types of
(foreign-centered) antigens, immune escape is inevitable. This is
because vaccinology still has not overcome the MHC restriction of
cytotoxic T cells, which is known to be essential for combating chronic
infections. Regarding prevention, HBV (hepatitis B virus) and HPV (human
papilloma virus) represent small exceptions since high Ab titers can
neutralize the virus before it enters target host cells. However, in
endemic situations, large-scale priming of antiviral Abs against these
viruses leads to immune escape again. Due to the lack of sterilizing
vaccines, we also lack curative (therapeutic) vaccines against chronic
or latent infections.
My argument aims to clarify
that ‘prevention of transmission’ is not necessarily an intrinsic
characteristic of a vaccine as A. Siri is erroneously suggesting. Hence,
the decision to remove certain vaccines from the current childhood
vaccination program should not be based solely on whether or not
existing vaccines can prevent transmission, but also on whether such limitations are determined by administration modalities and/or the epidemiological situation. Although the other vaccines A. Siri mentions cannot prevent pathogen transmission, this is not, in my opinion, a valid reason, or THE valid reason, to remove them from the schedule. THE
valid reason for urging global health authorities to stop polio
vaccination with the inactivated vaccine is that it is administered in a
context of circulating VDPV (vaccine-derived poliovirus), which
irrevocably causes immune escape — as shown in multiple publications.
The live attenuated vaccine was effective in
limiting wild poliovirus transmission, but because it was administered
orally, that live attenuated virus entered wastewater on a large scale.
Due to its high resistance to environmental factors, wastewater served
(directly or indirectly) as a reservoir for VDPV transmission, which
despite attenuation was still sufficiently virulent to cause more cases
of Vaccine-Associated Paralytic Polio (VAPP) than cases of paralytic
polio caused by wild poliovirus (reversion to virulence being only one
of the causes). Given that nearly one-third of the
world population—especially where polio remains endemic—lacks access to
clean drinking water, it is clear that the priority for global health should be providing clean water, not polio vaccination. Therefore, stopping this vaccination should be considered from a completely different perspective. Finally,
I find A. Siri’s concerns about tetanus vaccination unfounded. The goal
of such a vaccine was never to prevent bacterial transmission, but to
protect against the deadly and highly resistant neurotoxins produced by
the bacteria after spores from the environment insidiously enter the
body, preferably through small wounds or cuts (anaerobic conditions).
While one may debate the need to make this vaccine mandatory, I
personally continue to recommend it. I suspect A. Siri’s concerns stem
more from his aluminum phobia, which probably relates more to the autism
debate.
Hopefully, my reply once again illustrates the need for thorough scientific debate in which trained experts (not dilettantes) openly exchange views on this complex matters.
One-liners and black-and-white statements serve no one. Dissolving the
current ACIP is, in my opinion, a good step. However, it will be quite a
challenge to create a new, expert ACIP from the small circle of
independent scientists and vaccine specialists.
 By Independent News Roundup
By Independent News Roundup