 By Independent News Roundup
By Independent News Roundup

Before proceeding with this article, I strongly recommend first reading Part 1 (linked here),
Aussie17·15 OctRead full story
where I provided a comprehensive explanation of why Singapore’s mortality and drug sales data remain one of the most reliable and transparent indicators available for evaluating post-vaccination outcomes.
But before we get into that, as usual, please indulge me with a quick rant!
A friend in Singapore just sent me this heartbreaking story that came out yesterday on Channel NewsAsia.
It’s about Dr. Jessica Ee—a 34-year-old former model and dermatologist in Singapore. In August 2023, at age 32, she suffered a massive ischemic stroke that paralyzed the left side of her body, leaving her unable to move her left arm or leg, with her face drooping on one side. Just two months earlier, in June 2023, she’d had a warning transient ischemic attack (TIA, or “mini-stroke”) during dinner with friends, when she suddenly went mute for about 10 minutes—her mind racing but no words coming out—before recovering.
Doctors traced it to an undiagnosed patent foramen ovale (PFO), a small hole in the wall between the top two chambers of her heart that she was born with. This is common—about 1 in 4 adults has a PFO and never knows it, as it usually causes no issues—but in her case, it allowed a blood clot to slip from the right side of her heart (likely from the veins, such as the legs) across to the left side, bypassing the lungs’ natural filter and traveling straight to her brain, where it blocked a major artery in what’s known as a paradoxical embolism. The article doesn’t specify why the clot formed in the first place but simply blamed the hole in her heart. Again, 25% of the general population has this hole and most of them don’t get stroke.
Two years later, she’s still in intensive recovery: she walks only with great effort using a cane, her speech is slow and deliberate, and while she regained swallowing after about a month, basic independence like showering remains a daily challenge.
That said, I would never claim that Dr. Jessica Ee’s stroke was “definitely caused by the vaccine,” because strokes in the young are almost always multifactorial, and we will probably never know the exact weight of every trigger in her individual case (*cough* genetic *cough* vaccines).
However, during Singapore’s intense 2021 vaccination drive—when public skepticism was running high, including from everyday workers like Mr Cedric Lim who feared the experimental mRNA shots due to their untested risks but were coerced into getting jabbed just to keep their jobs and access basic necessities like grocery shopping, and from more outspoken figures like Ms Iris Koh who was loudly warning of “vaccine genocide” on her Telegram channel “Healing The Divide” and organising protests, and the government had just announced that unvaccinated people could no longer enter malls or dine in restaurants—Dr Jessica Ee went on Facebook to gloat, posting: “I am loving the meltdown of the anti-vaxxers.”

I take no pleasure in a 34-year-old woman spending her days re-learning how to swallow and walk. Watching her force a smile through slurred speech while clutching a cane breaks my heart just as it should break yours.
But that is exactly why this story must be seared into the conscience of every doctor who, in 2021, chose cruelty over compassion. As a doctor, your first oath is to the terrified mother clutching her healthy teenage son, the young nurse who just wants to keep her fertility, the father who watched his own brother die of a heart attack at 40, people who looked at a brand-new genetic mRNA shot and whispered, “I’m scared.”
When those human beings begged for pause, for answers, for even a shred of humility from the white-coat class, the very last thing they deserved was a physician mocking them on Facebook with “I am loving the meltdown of the anti-vaxxers.” That wasn’t medicine. That was cruelty dressed in arrogance.
Imagine laughing at their fear in 2021… and then, two years later, waking up at 32 unable to move half your body, unable to speak, unable to swallow, unable to hug your own mother because a clot slipped through a hole in your heart and stole everything in an instant. Imagine scrolling back to your own smug post while lying paralysed in a rehab ward, the laughter now echoing in your own skull like a scream you can’t get out. That is the price of trading empathy for applause.
Now, almost 5 years later, the FDA have declared has taken a step of historic proportions. For the first time since the vaccines were rolled out, the FDA has officially acknowledged that the mRNA injections caused the deaths of at least ten children among the 96 paediatric cases it examined in detail. At least 10 families lost a child after the COVID vaccines and imagine some doctors mocking them and was “loving the meltdown of antivaxxers”.
The admission is contained in an internal memorandum written by Vinay Prasad, M.D., M.P.H., who currently holds the position of Chief Medical and Scientific Officer (CMSO) at the FDA—a role that combines the agency’s highest medical and scientific leadership responsibilities. Dr Prasad simultaneously serves as Director of the Center for Biologics Evaluation and Research (CBER), the division entrusted with regulatory oversight of all vaccines and biological products in the United States.
This is therefore not a junior official’s footnote or an informal comment; it is a formal statement from the individual occupying the two most senior scientific and medical positions responsible for vaccine safety within the FDA itself.
You can scroll down all the way below to read the full memo (subheader under U.S. Food and Drug Administration Center for Biologics Evaluation and Research
MEMORANDUM). Or simply review my key highlights for the essential points.
But before we get into that, let me show you the drug sales data for post-stroke patients in Singapore over the last 10 years.
Fractionated heparin — more commonly known as low-molecular-weight heparin (LMWH), with brand names like enoxaparin (Clexane/Lovenox) or dalteparin (Fragmin) — has been on the market for over 30 years and is today the world’s most widely used blood thinner for preventing clots. It works like a smart, longer-acting version of old-fashioned heparin: it grabs onto a natural brake in your blood (antithrombin) and mainly stops one key clotting engine (factor Xa), so blood still flows but dangerous clots are much less likely to form in the legs or lungs. After a stroke, when patients can’t move much and are at high risk of these life-threatening clots, doctors give a simple once-a-day injection under the skin — no blood tests needed. In modern stroke units worldwide, about 55–65 % of all immobilized stroke patients receive fractionated heparin for this clot-prevention role (the rest get alternatives like fondaparinux, very low-dose DOACs, or — in a minority — old-style unfractionated heparin). Despite no big new medical reasons or guideline changes since 2023, we’ve seen a mysterious sharp rise in its use from late 2023 onward.
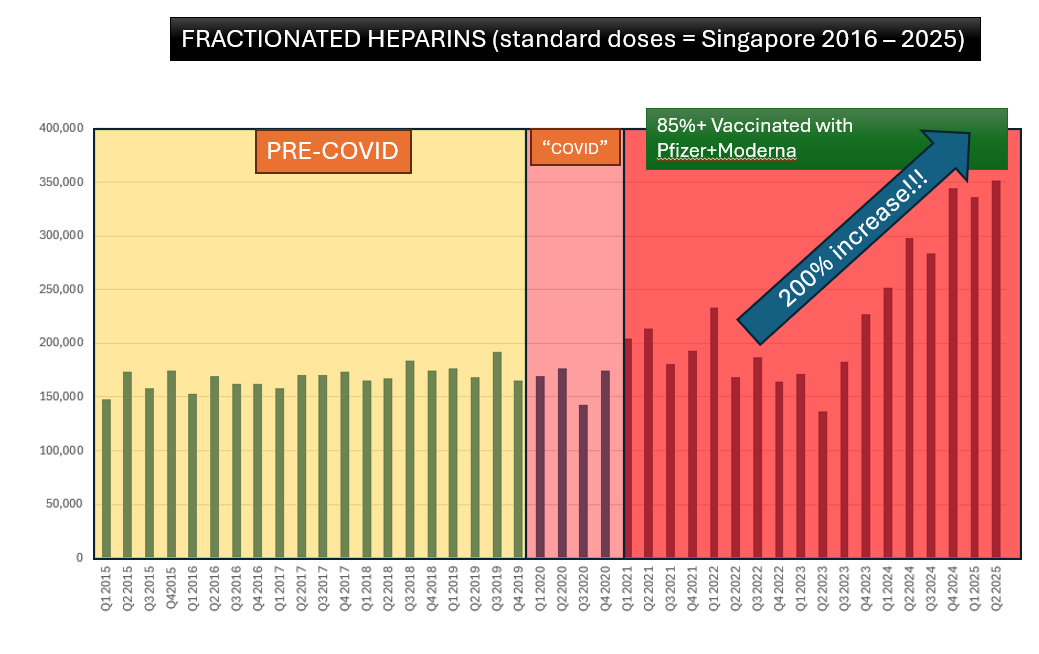
So while the headlines were screaming about “unexplained” surges in strokes and clotting in young, healthy people, the stroke wards were quietly started burning through fractionated heparin faster than at any point since the 2015… just to stop today’s stroke patients from throwing the next clot.
I find this quite concerning because the sharp rise in heparin use begins more than 30 months after most Singaporeans received their third COVID-19 vaccine dose. Very few studies have looked at strokes to vaccination after such a long delay — almost all reported cases occur within days to weeks of the shot. Interestingly, the same graph also shows smaller spikes (roughly 20–50 % increases) between Q1 2021 and Q1 2022, which do line up with the main vaccination and booster rollout periods.
The closest study I could find is a 2025 Japanese paper that examined brain tissue from 19 women who suffered or died from hemorrhagic strokes between 2023 and 2024.

Using special staining techniques, the researchers detected vaccine-derived spike protein inside the walls of cerebral blood vessels in 8 of these patients — in one case still present 17 months after her last mRNA shot, and in others at 11–12 months. None had active COVID-19 infection at the time, pointing to the vaccine (not the virus) as the source of the spike. Wherever the spike protein was found, the vessel walls showed inflammation and damage.
Anyway, that’s all for now. Here is the memo from the FDA acknowledging that at least 10 children out of the 96 analyzed died from the vaccines.
To: CBER Leadership Team
From: Vinay Prasad, MD, MPH
Chief Medical Officer
Dear Team CBER,
I am writing to report that OBPV career staff have found that at least 10 children have died after and because of receiving COVID-19 vaccination. These deaths are related to vaccination (likely/probable/possible attribution made by staff). That number is certainly an underestimate due to underreporting, and inherent bias in attribution. This safety signal has far reaching implications for Americans, the US pandemic response, and the agency itself, which I wish to discuss here. I also want to address some frequent objections.
Prior to joining the US FDA, the FDA Commissioner closely followed reports of vaccine-induced myocarditis. Unlike the COVID virus, which has a steep age gradient-- being at least 1000 times more likely to kill an 80 year old than an 8 year old-- myocarditis appeared to have the opposite pattern. Young, healthy boys and men-- those least likely to experience bad covid outcomes-- bore the greatest risk. The risk was as high as ~200-330 per million doses given in the highest risk demographic groups. Notably, the US FDA and CDC were not the first to recognize the safety signal-- instead the Israelis were-- and worse in May of 2021, then CDC director Rochelle Walensky stated, “We have not seen a signal and we’ve actually looked intentionally for the signal in the over 200 million doses we’ve given,” Many felt this statement was dishonest and manipulative.
The Commissioner, senior advisor Tracy Beth Hoeg MD PhD, myself and colleagues demonstrated that COVID-19 boosters, and the accompanying mandates by colleges, were on balance harmful to young men in a widely discussed, peer reviewed paper in 2022. Like many academic physicians, we felt the FDA and CDC abdicated their duty to the American people. These agencies did not quickly attempt mitigation strategies such as spacing doses apart, lowering doses, omitting doses among those with prior COVID-19.
Worse, the FDA delayed acknowledgement of the safety signal until after it could extend marketing authorization to younger boys 12-15. This is described by the Commissioner and I in JAMA. Had the acknowledgement come early, these younger boys, who likely did not require COVID-19 vaccination, may have chosen to avoid the products.
In the summer of 2025, Dr. Hoeg began investigating VAERS reports of children who had died after administration of the COVID-19 vaccine. By late summer, she had concluded that there were in fact deaths-- a fact this agency had never publicly admitted.
Dr. Hoeg organized a small meeting to discuss these deaths with OVRR and OBPV stakeholders. The slides she presented, emails she sent, and distorted firsthand reports was shared with media outlets. The general narrative was that OVRR staff disagreed with Dr. Hoeg’s assessment that the deaths were due to vaccine receipt. Some staff present who leaked portrayed the incident as Dr. Hoeg attempting to create a false fear regarding vaccines.
I then asked OBPV to perform a detailed analysis of deaths voluntarily reported to the VAERS system-- in full interest of balance. Causality is easy to assess in a randomized trial, but with case reports, causality is typically assessed on a subjective scale. In this scale ranging from certain to unlikely-- certain, possible/likely, and probable are broadly considered as related to the product.
The team has performed an initial analysis of 96 deaths between 2021 and 2024, and concludes that no fewer than 10 are related. If anything, this represents conservative coding, where vaccines are exculpated rather than indicted in cases of ambiguity. The real number is higher.
This is a profound revelation. For the first time, the US FDA will acknowledge that COVID-19 vaccines have killed American children. Healthy young children who faced tremendously low risk of death were coerced, at the behest of the Biden administration, via school and work mandates, to receive a vaccine that could result in death. In many cases, such mandates were harmful. It is difficult to read cases where kids aged 7 to 16 may be dead as a result of covid vaccines.
Did COVID-19 vaccine programs kill more healthy kids than it saved?
We do not have reliable data estimating the absolute benefit (absolute risk reduction) regarding severe disease and death in healthy children from vaccine receipt. OVRR and OBPV rely on observation cohort or case control data with notorious methodologic biases. FDA has never requested the manufacturers demonstrate in randomized fashion that vaccinating children. improves these outcomes. The available randomized data in children is deeply limited, and broadly negative for symptomatic infection, as discussed in prior ad-coms. Furthermore, COVID-19 was never highly lethal for children, and now MIS-c has decreased drastically, and the harms, to kids, are comparable to many respiratory viruses for which we do not provide annual immunization.
Comparing the number of kids who died from COVID against these deaths would be a flawed comparison. We do not know how many fewer kids would have died had they been vaccinated, and we do not know how many more kids died from taking vaccines than has been voluntarily reported. Instead, the truth is we do not know if we saved lives on balance.
When it comes to vaccine deaths, VAERS is passively reported. It requires a motivated person, often a doctor, to submit the information. The submission process is tedious and most people who start the form give up along the way. Many more deaths may be unreported. Finally, the FDA has failed to properly enforce many required post market commitments for COVID-19 vaccines, including for pregnant women and to document subclinical myocarditis.
Putting these facts together, it is horrifying to consider that the US vaccine regulation, including our actions, may have harmed more children than we saved. This requires humility and introspection.
Why did it take the FDA Commissioner to identify these deaths?
There is no doubt that without this FDA commissioner, we would not have performed this investigation and identified this safety concern. This fact also demands serious introspection and reform. Why were these deaths not actively reviewed in real time? Why did it take until 2025 to perform this analysis, and take necessary further actions? Deaths were reported between 2021 and 2024, and ignored for years.
I suspect the answer is cultural and systemic. I have no doubt that many vaccines have saved millions of lives globally, and many have benefits that far exceed risks, but vaccines are like any other medical product. The right drug given to the right patient at the right time is great, but the same drug can be inappropriately given, causing harm. The same is true for vaccines. The US government’s coercive and unethical covid-19 vaccine mandates in young people may have been harmful. In contrast, there is no doubt that an elderly, un-immune American benefitted from Doses 1 and 2 in 2020. The people who might have benefit most from vaccination were those too old to be affected by workplace mandates-another Biden administration blunder.
Does COVID cause more myocarditis than covid vaccines?
A perennial argument is that COVID 19, the virus, causes more myocarditis than COVID-19 vaccines. In fact, I heard this argument made inside CBER recently when one company submitted their PMC. Here is why that argument is wrong.
In order to study how often people have myocarditis after the virus, you would want to collect everyone who got covid, and see how many get myocarditis. Yet, studies on this topic don’t do this. They take people who presented to health care systems and had covid-19 and ask how many have myocarditis. But we all know most people who get covid simply recover at home. People who seek medical care are the sickest ones. These studies use a false denominator.
Second, the demographic matters. I have no doubt COVID vaccines were life saving for an 80 year old who never had COVID, but should a 20 year old get his 6th dose this fall? These studies often fail to look at the balance in younger people.
Finally, you still get COVID anyway. No amount of covid vaccines stops a person from getting covid, so the risk is not virus vs vaccine. It is vaccine + virus vs virus alone.
I am not aware of any analysis that does this right, and we have performed an empirical review of this fact.
Thoughts on CBER staff who are leaking to the media
I have no doubt that individuals who are providing media outlets with slides, emails and personal anecdotes believe they are doing the right thing. Unfortunately, this behavior is both unethical, illegal, and, as this case illustrates, factually incorrect. COVID-19 vaccines did result in the death of children. Dr. Hoeg was correct in her assessment-- any small differences in opinion about specific cases are due only to the fact that subjective attribution of death is inherently a topic where reasonable people may have subtle disagreements. But the overall order of magnitude and directionality show concordance between Dr. Hoeg and long-time CBER staff.
Drs. Gruber and Krause resigned in 2021 as Director and Deputy Director of OVRR
Finally, one fact that must be mentioned is that disagreements by my predecessor and career staff had led to resignations in the past. Drs. Gruber and Krause ran the vaccine division for decades. They resigned over two issues: Dr. Marks insisted that annual boosters should be for all people--irrespective of age and risk-- while Gruber and Krause preferred a risk based, evidence based approach. And Dr. Marks pushed through a BLA for the COVID-19 shots, which permitted the Biden administration to administer unethical COVID-19 mandates.
As a professor, I agreed with Gruber and Krause. Furthermore, there have been prior CBER directors who have held this chair and had fundamentally different views. Some have felt the CBER director should override reviewers to approve gene therapies that do not work because of patient demand. When these products later result in post market deaths, it is difficult to take corrective action. I favor approving products with benefits that exceed risks.
Incentive in vaccine making
It is well acknowledged that the FDA does not consider the cost of drugs in our approval decisions, and similarly it is not our role to lower evidentiary standards or mask safety concerns to create artificial financial incentives to make vaccines. That said there are unique financial incentives for vaccine markers.
Covid-19 vaccines earned 100 billion dollars globally. The annual US vaccine market is estimated to be over 30 billion dollars, projected to pass 50 billion in a decade, and a single new vaccine for pregnant women has industry analysts estimating 1 billion a year in annual returns.
Additionally, vaccines do not go “generic.” There is no biosimilar pathway. You can’t show your biosimilar vaccine has the same antibody titer and get approval. This means two things: companies can expect long tails of earnings, and FDA acknowledges that cell and humoral immunity surrogates are insufficient for generic approvals-- a position I agree with.
The fact that we don’t offer generic or biosimilar vaccines because no amount of cell or humoral mediated immune surrogates would mean that a product retains efficacy has a deeper logical conclusion: how can we accept such endpoints to approve entirely novel products?
The path forward for CBER/OVRR/OBPV
I want to outline a path forward. Our general approach in CBER will be to direct vaccine regulation towards evidence based medicine. This means: we will take swift action regarding this new safety concern, we will not be granting marketing authorization to vaccines in pregnant women based on unproven surrogate endpoints (any prior promises will be null and void), and we will demand pre-market randomized trials assessing clinical endpoints for most new products. Pneumonia vaccine makers will have to show their products reduce pneumonia (at least in the post-market setting), and not merely generate antibody titers. Immunogenicity will no longer be used to expand indicated populations-- these populations should be included in premarket RCTs.
We will revise the annual flu vaccine framework, which is an evidence-based catastrophe of low quality evidence, poor surrogate assays, and uncertain vaccine effectiveness measured in case-control studies with poor methods. We will re-appraise safety and be honest in vaccine labels. I look forward to hearing your thoughts on how to do this better.
Additionally, at FDA, we have not been focused on understanding the benefits and harms of giving multiple vaccines at the same time. This is a concern shared by many Americans. The FDA’s standard has been to require randomized studies too small to draw any conclusions from-- creating a false sense of efficacy and safety.
OVRR and OBPV staff will be tasked with writing guidelines to reflect these changes, and the mission of CBER will change to reflect this worldview. Never again will the US FDA commissioner have to himself find deaths in children for staff to identify it. Vaccines will be treated like all other medication classes-- no better or worse than AAV vectors, monoclonal antibodies, or anti-sense oligonucleotides.
Insofar as vaccines have third party benefits, and many do, these will be judged just like drugs may have third party benefits-- a person who takes an appropriate psychiatric medicine may be a better parent or spouse-- but this requires data and cannot be assumed. I have seen no evidence that COVID-19 vaccines, which do not halt transmission, benefit third parties. I have no doubt that MMR vaccines do provide third party benefits when administered to high enough fractions of society.
Having said this, I remain open to vigorous discussions and debate on these topics, as I have always been. I am open minded to modifications or alterations. As you can imagine, I believe these debates should be private, internal to FDA, until they are ready to be made public. I don’t endorse selective reporting of our meetings and documents. Some staff may not agree with these core principles and operating principles. Please submit your resignation letters to your supervisor and CC my deputy Katherine Szarama.
For those who choose to remain in CBER, I look forward to working with you, learning from you, discussing with you, and interacting with you on our shared mission: to elevate vaccine science to 21st century evidence based medicine.
Vinay Prasad MD MPH
Signing off for now
A17
